A Vaccine to End the Quarantine:
The complex process of a SARS-CoV-2 vaccine, from petri dishes to humans.
 The question of the SARSCoV-2 (COVID-19) vaccine release date lingers in the air as individuals slide into the seventh month of social distancing and in some cases, complete quarantine.The complex process of vaccine development and testing can vary from two months to 15 years; according to the Centers for Disease Control and Prevention (CDC), it’s estimated that a vaccine may be ready by early November 2020.
The question of the SARSCoV-2 (COVID-19) vaccine release date lingers in the air as individuals slide into the seventh month of social distancing and in some cases, complete quarantine.The complex process of vaccine development and testing can vary from two months to 15 years; according to the Centers for Disease Control and Prevention (CDC), it’s estimated that a vaccine may be ready by early November 2020.
The last pandemic, the 2009 Swine Flu, was caused by the H1N1 influenza virus, and it took around three months to create and start distributing the vaccine for this variant of the influenza virus.
The medical and scientific community has decades of experience creating the flu vaccine against different influenza strains, so the framework to create the vaccine was already present.
While the scientific community was able to develop the Swine Flu vaccine faster, the community has never before created an effective vaccine against COVID-19, which explains why we still don’t have a vaccine after six months. At the same time, viruses such as HIV and the common cold still do not have a vaccine; the viruses only have treatments to keep the disease manageable.
Normally, one would assume that the timeline to develop a COVID-19 vaccine may be extended, as the scientific community has never developed a vaccine against coronavirus before. However, the pressure to create a vaccine amidst the pandemic may cause this vaccine to differ from other vaccines.
Ryan Sandvig, a clinical trial professional with 15 years of clinical research experience, has noticed the same.
“The [SARS-CoV-2] timeline is much faster than we normally do clinical trials,” Sandvig said. “They are compressing something that generally takes 10-15 years in 1-2 years. We did have a headstart with vaccine development because of the first SARS virus, but since the pandemic was quickly controlled, research moved from a coronavirus vaccine development to other areas of interest.”
According to the World Health Organization (WHO), “There are currently over 169 COVID-19 vaccine candidates under development, with 26 of these in the human trial phase.”
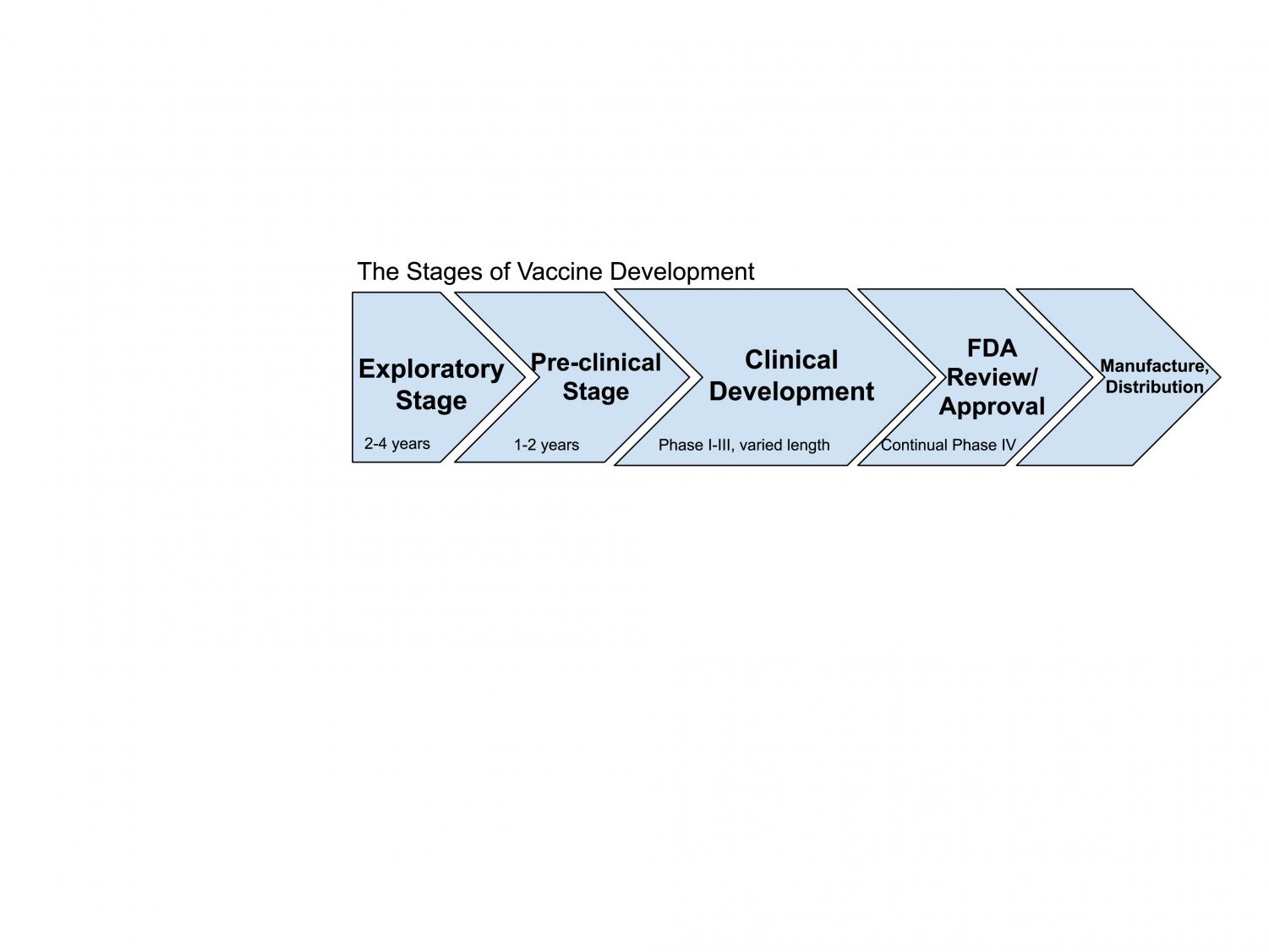
The phases undertaken for the development of a vaccine, according to the CDC, begin with the Exploratory Stage, in which basic laboratory research is conducted over a period of four to five years. In this stage, funding from scientific and governmental organizations is sought.
In terms of a COVID-19 vaccine, this step can be quickly completed as the government and various organizations have supported the vaccine to be researched as quickly as possible.
The Preclinical Stage, in which non-human testing occurs, follows suit. If the vaccine passes this stage, it’s onto Clinical Development, which is composed of three main phases: Phase I-III.
In Phase I, there is a small number of patients, in which researchers are “very closely watching each patient to see what side effects they have from the vaccine, and if it looks promising they will go onto phase II and III,” said Sandvig.
In Phase II, the research involves a greater number of patients, where researchers can get a better sense on the vaccine’s safety.
In Phase III, thousands of patients participate, and researchers are looking at if the vaccine is safe enough, if the benefits outweigh the risks and how effective the vaccine is.
The vaccine then goes through the regulatory review and approval, manufacturing, quality control, distribution and education, sales, and marketing.
The need and interest in developing the COVID-19 vaccine has allowed for certain process modifications that can reduce the vaccine development timeline, including the time reduction between each phase and manufacturing the vaccine before the vaccine is approved. If the vaccine passes Phases I-III and gains approval, then the ongoing Phase IV studies take place.
In Phase IV, formal vaccine studies occur continually and act as a safety program in checking for and assessing for side effects of the vaccine, which are reported through the Vaccine Adverse Event Reporting System (VAERS).
“In a regular clinical trial, you give an experimental treatment to someone today and it may take a year or multiple years for there to be an adverse event,” said Sandvig. “Due to the gravity of the situation, we don’t have the luxury of time to wait and see all the potential long-term adverse events.”
Then the discussion of distribution blooms, in which healthcare workers, the immunocompromised, and essential workers fall to the front of the line. Bahareh Khatibi, a California physician, said it makes sense to offer vaccination to certain groups first, but she sees another issue within this.
“Will the vaccine be a recommendation or a mandate?” said Khatibi. “With the unprecedented speed with which we are creating and testing these vaccines, could we be missing serious long term, adverse events?”
It’s reasonable to question the validity of a highly demanded, time-sensitive vaccine, especially in the political climate we have today, with the concerns that the administration could be influencing the CDC and the Food and Drug Administration (FDA).
The FDA has the ability to grant an Emergency Use Authorization for the vaccine without having finished trials, under the assumption that the FDA has reviewed a significant amount of data. In the past they have made errors, such as approving the use of hydroxychloroquine, whose authorization was revoked after emerging studies disproving its effectiveness.
“When the states report their COVID-19 numbers, they are required to send them to the White House before the CDC, which is unusual,” said Sandvig.
“Before July, the CDC got the numbers first. Election year means numbers and data can get politicized, but we can only hope that the vaccine reporting is unbiased and factual, and that it’s created and distributed soon.”
Aurora Khatibi Garrity (11) is a staff writer and member of the social media team for The Point! At PVHS, she is excited and ready for a year of growth...